Share:
Should implants go in front or behind the muscle?
Implants can go either above or behind the muscle. We’ll explore whether in front or behind the muscle is best.
Implants can go either above or behind the muscle. We’ll explore whether in front or behind the muscle is best.

When you have your breast augmentation surgery, your surgeon has to create a space where your implants will sit. This space is called a “pocket” and there are a few possible places where your surgeon can make this pocket.
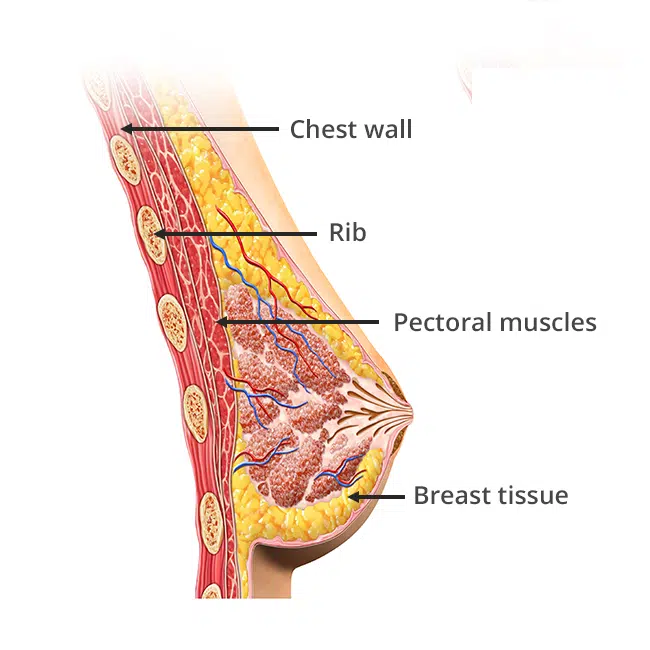
You may have heard about “in-front-of-the-muscle” or “behind-the-muscle” placement. The muscle that we are talking about is the “pectoralis major” muscle, which you can see when someone “flexes their pecs”. The “pec” muscle lies underneath your breast tissue and right on top of your rib cage. Each “pocket” option has its own advantages and disadvantages, so let’s talk about them.
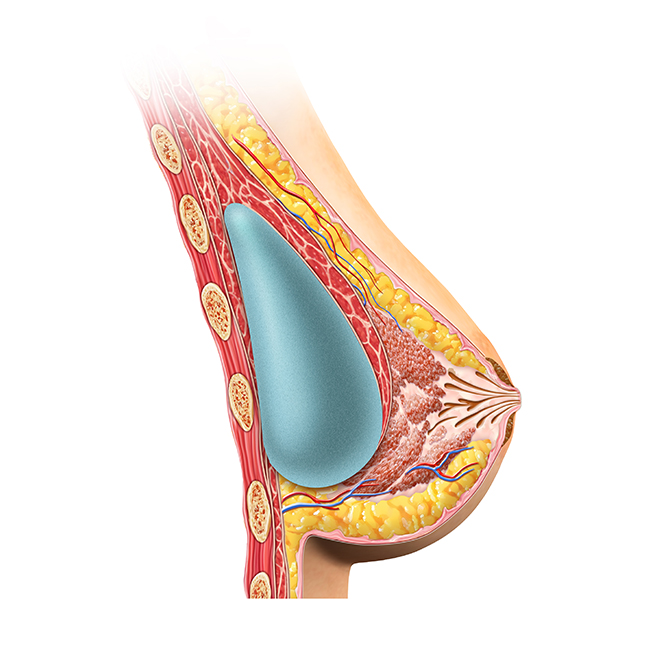
The subglandular method is also called “submammary”, “in-front-of-the-muscle” and “over-the-muscle”. Here, the pocket is created directly beneath your breast tissue. In this approach, your implants will sit beneath the breast tissue and on top of the pec muscle.
This pocket doesn’t involve as much tissue dissection as other approaches, so typically surgery time is shorter. Because the muscle is not affected, you won’t have as much soreness with this pocket. Your recovery time will be shorter and you’ll be able to return to your normal activities sooner. Because the implants sit on top of the chest muscle, there usually isn’t any distortion or visible movement of the implants when your chest muscle contracts. This option might be good for women who have very well developed pec muscles from working out, like professional body builders.
There are also some cases where a woman’s breast shape is tubular or conical. In these cases, it can help to go subglandular to try to improve the shape. This also holds true for women that have mild breast sagging. Subglandular may give a little bit of a lifted shape, without having to go through a formal breast lift surgery. The key words are “a little bit lifted”. Many women will want more lifting than a subglandular breast augmentation alone can provide.
One of the major disadvantages to a subglandular placement is the high rate of capsular contracture.1
This may be due to the presence of bacteria that normally live in your breast’s mammary glands. If the bacteria somehow escapes the ducts during implant placement, it can colonize the implant surface and create a biofilm, which may contribute to the development of capsular contracture.2
Another disadvantage is, that in patients with thin skin, you can see visible rippling around the implant edges, and the implant may be very easy to feel beneath the tissue. If you get rippling on the top of your implants, this may be visible if you’re wearing a low-cut top. Also, because the implants sit immediately beneath the breast tissue, patients with these implants may have a more difficult time with getting mammograms.
Fascia is a thin layer of tissue that covers muscles. A subfascial implant placement involves the separation of this layer from the top of the pec muscle to create the implant pocket.
Some surgeons prefer this approach because it has lower instances of capsular contracture, rippling, and palpability than a subglandular approach.3
This downsides to this method is that it usually results in bloodier surgery and longer surgery times. It’s also very common for this extremely thin fascia layer to become injured and broken, resulting in what actually turns out to be subglandular placement. If that happens (and you may not know about it), you will be subject to the same downsides of the subglandular approach, namely, increased capsular contracture and rippling.
The subfascial approach is much less commonly performed in the United States than the other two approaches.
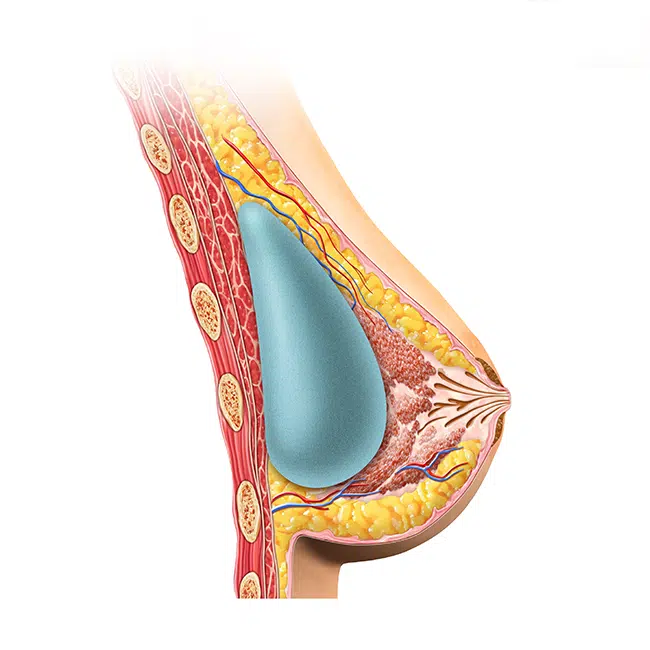
The subpectoral approach is also called “submuscular”, “behind-the-muscle” and “under-the-muscle”. In this case, the pocket is created beneath the pectoralis chest muscle. In the past, many implants were done with the subglandular approach but the rippling and capsular contracture that was seen long term was a real problem. This led to the subpectoral approach becoming the preferred method for many surgeons in the United States because of its major advantages.
The main advantage of the subpectoral approach is a lower chance of capsular contracture.4
This is thought to be due to the muscle’s movement over the surface of the implant, which can disrupt the formation of a thick capsule. Also, because implants are placed below the muscle, there is an extra layer of tissue coverage to decrease visible rippling and feel-ability. This approach also makes mammography easier because it keep the implant further away from the breast tissue.
The downsides of subpectoral is that you can be more sore during the recovery period because of the muscle work that has been done. Just keep in mind that putting up with a few extra days of soreness with subpectoral is worth it, if you can avoid some of the long term problems that come with subglandular. Another potential issue is that, especially if you have well-developed pec muscles, you may notice movement of your implants when you “flex your pecs”.
One popular option is a variation of the “subpectoral” approach, called “dual plane”. You can basically think of it as “subpectoral”, except that the lower part of the implant will be subglandular. Many surgeons consider it the “best of both worlds”. This approach leads to a natural appearing breast and avoids some of the problems of purely subglandular and submuscular approaches. Its disadvantages will be the same as the subpectoral approach.
These days, most women have their implants placed subpectoral or “dual plane” because of the advantages that you just read about. Some women with certain breast shapes may choose to go subglandular.
Since each approach has its pro’s and con’s, you can go over each option when you see your plastic surgeon for a consultation. They will listen to your wishes, look at your anatomy, and, together with you, decide on which pocket placement would work best for you.
Our board certified plastic surgeons can discuss with you the options for breast implant placement. After going over what you wish for, one of our doctors will measure and examine your breast and chest to help you pick the best chose for your body type.